SCREEN 01
AI interpretation card
Coder · chart review queue
SCREEN 02
Coder override interface
Coder · condition correction
SCREEN 03
Enrollment segmentation dashboard
Enrollment analyst · plan assignment
SCREEN 04
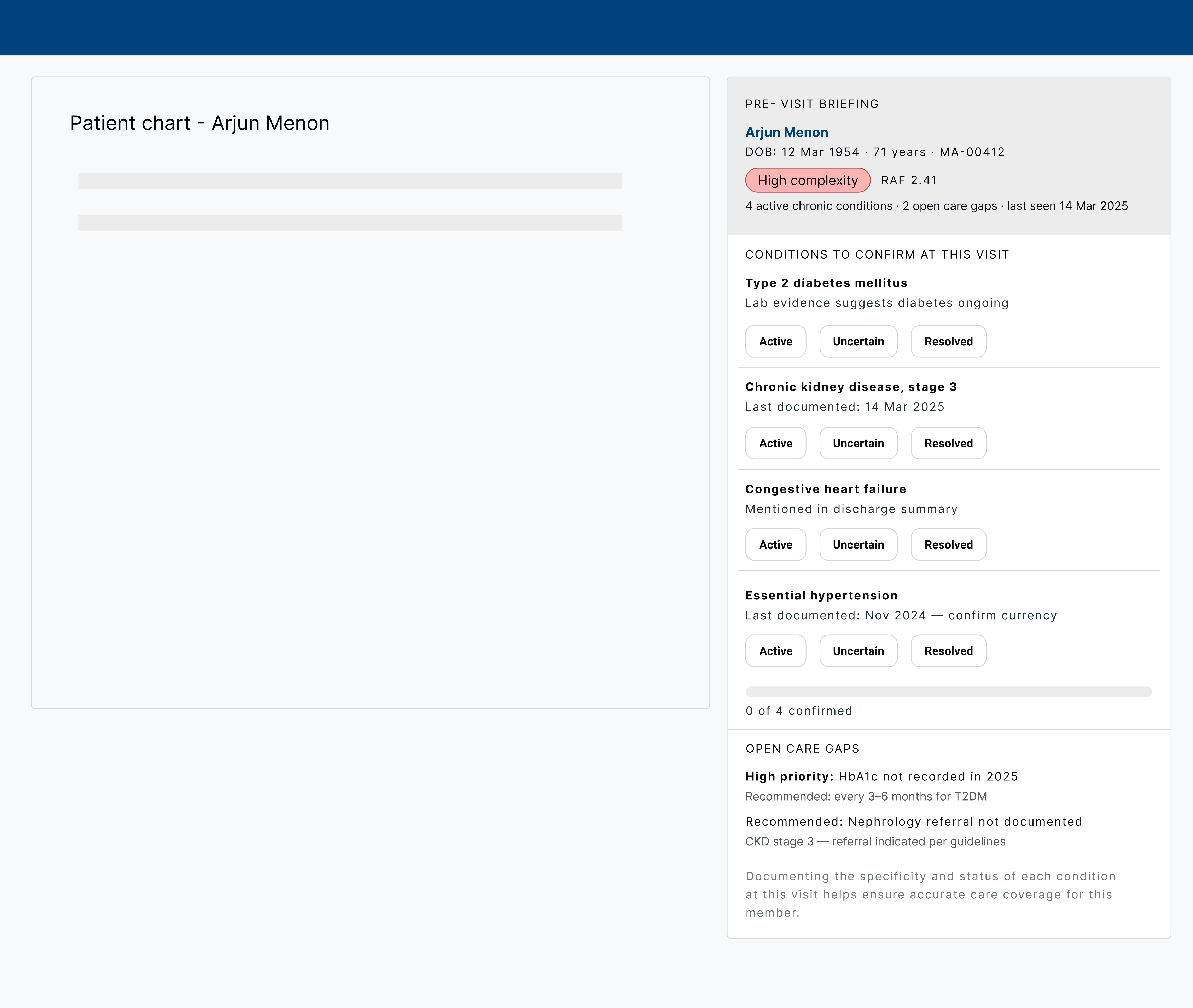
Provider pre-visit briefing
Physician · EHR embedded panel
Screen 01
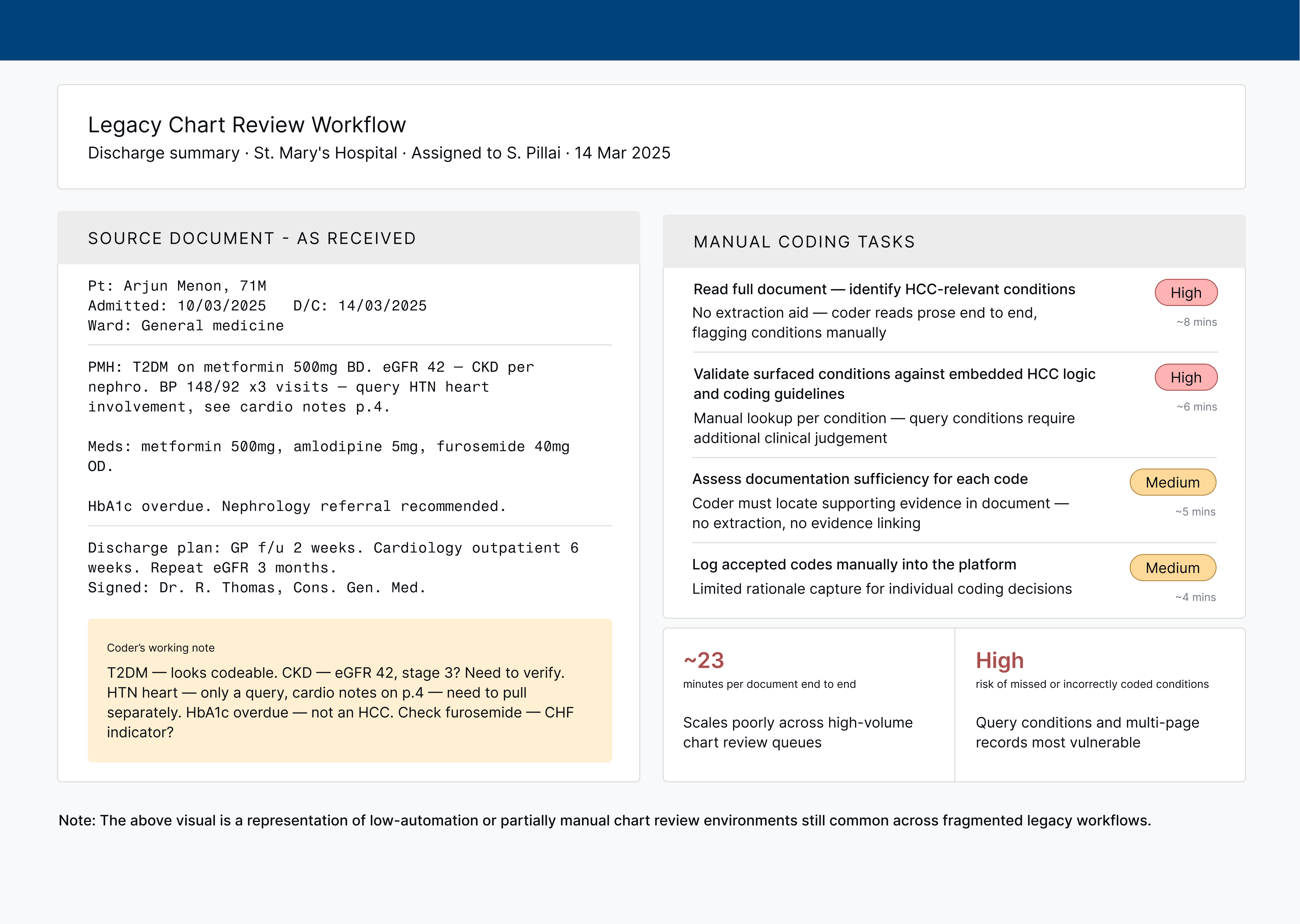
AI interpretation card — chart review queue
[ Screen 01 — drop export here ]
Each scanned document produces one card. Three conditions are flagged from a discharge summary: Type 2 diabetes mellitus at high confidence (94%), CKD stage 3 rejected with a reason ("not sufficient for coding"), and hypertensive heart disease at 61% needing review. Each flag shows the exact evidence snippet from the source text and an Accept / Reject / Add note action set. Coders can bulk-accept all high-confidence flags at the bottom without reviewing each individually.
Screen 02
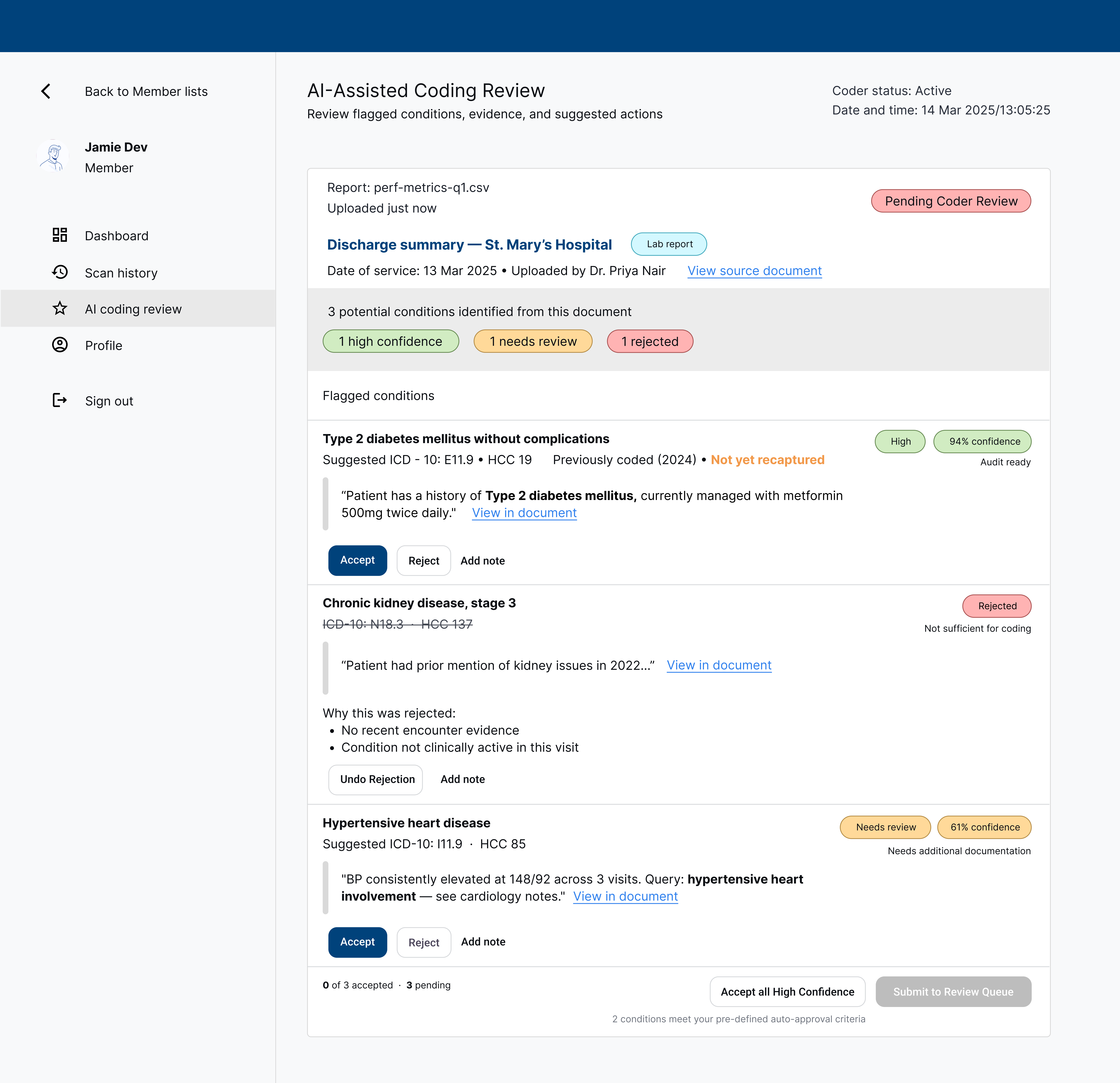
Coder override interface — inline correction
[ Screen 02 — drop export here ]
Override expands inline, no modals or navigations away from the queue. A required reason dropdown surfaces five options: not documented in this record, condition already coded, insufficient clinical evidence, incorrect code suggested, and other. Selecting "Incorrect code suggested" would reveal a code substitution field, feeding a correction signal back to the AI model. Friction is calibrated to the flag's confidence, whereby high-confidence overrides require a reason; lower-confidence ones do not.
Screen 03
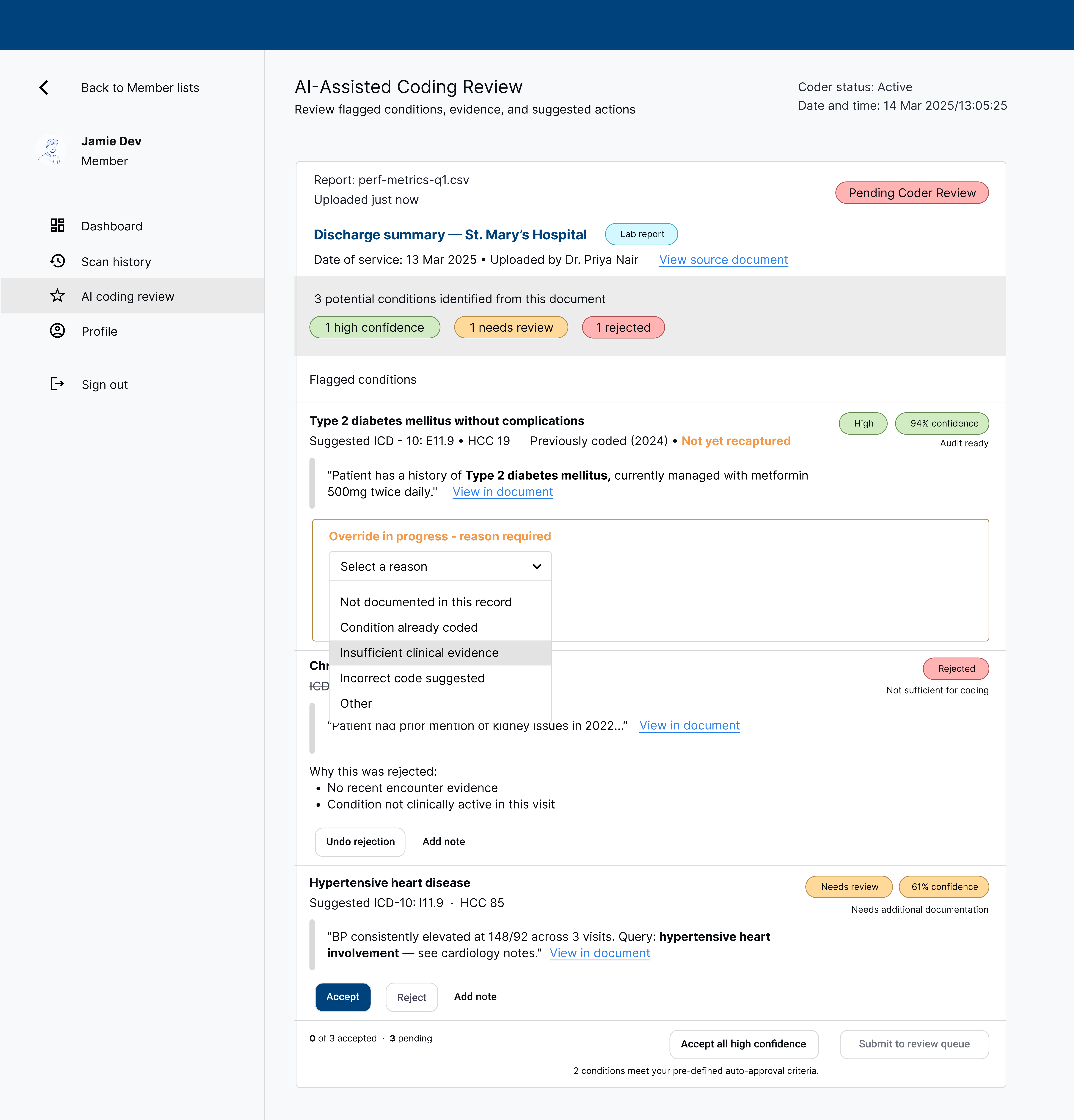
Enrollment segmentation dashboard — shared view
[ Screen 03 — drop export here ]
Shared by risk adjustment and enrollment ops. Four KPI tiles surface the pipeline at a glance: 247 members pending segmentation, 84 high risk, 12 flagged for critical review, and a 91% HCC gap closure rate. Each member row shows risk tier, gap status, and plan match. Expanding a row (shown for Arjun Menon) reveals the RAF score bar, confirmed HCC codes, and a plan match recommendation with confidence score. There are all actionable with Confirm, Export, or Override.
Screen 04
Provider pre-visit briefing — EHR embedded panel
[ Screen 04 — drop export here ]
A sidebar panel embedded in the existing EHR alongside the patient chart. No ICD-10 codes are visible, except for condition codes, keeping the frame clinical rather than billing-oriented. Four conditions are listed with Active / Uncertain / Resolved toggles for the provider to confirm currency at the visit. Below, two open care gaps are framed as clinical recommendations: a high-priority HbA1c flag and a nephrology referral. The CDI nudge appears last, after clinical context has established trust.